
¤
¤
¤
POZOR! Nije za svakoga sadržaj…
Mogli biste izgubit sebe gledajući istine o otvorenom (dozvoljenom!?)
ubijanju djece – prijavljeno preko 1100 koji su umrli od cijepljenja,
a ukupno je 4.4 TISUĆE roditelja isplaćena odšteta u iznosu od 3 MILIJARDE dolara.
Naslov sa youtubea:
(hrv: CDC zviždač govori kongresu
o UZROKU AUTIZMA – cjepivo)
CDC Whistleblower Told Congress of Coverup on Vaccines Causing Autism
Pozor! Mogli biste izgubit sebe gledajući istine o otvorenom (dozvoljenom!?)
ubijanju djece.
Da li cijepljenje potiče nastajanje autizma? CDC liječnica na kongresnom saslušanju.
Na sudu dokazano da MMR vakcina/ cjepiva izaziva velika oštećenja! (i smrt)
Ovo je NA ENGLESKOM TEXT, sa informacijama od Harvarda.

Harvard Trained Immunologist Demolishes California Legislation That Terminates Vaccine Exemptions
The following open letter by a PhD Immunologist completely demolishes the current California legislative initiative to remove all vaccine exemptions. That such a draconian and cynical state statute is under consideration in the ‘Golden State’ is as shocking as it is predictable. After all, it was mysteriously written and submitted shortly after the manufactured-in-Disneyland measles ‘outbreak’.
 The indisputable science that is employed by Tetyana Obukhanych, PhD ought to be read by every CA legislator who is entertaining an affirmative vote for SB277. Dr. Obukhanych skillfully deconstructs the many false and fabricated arguments that are advanced by Big Pharma and the U.S Federal Government as they attempt to implement a nationwide Super-Vaccination agenda.
The indisputable science that is employed by Tetyana Obukhanych, PhD ought to be read by every CA legislator who is entertaining an affirmative vote for SB277. Dr. Obukhanych skillfully deconstructs the many false and fabricated arguments that are advanced by Big Pharma and the U.S Federal Government as they attempt to implement a nationwide Super-Vaccination agenda.
When the California Senate refuses to consider authoritative scientific evidence which categorically proves the dangerous vaccine side effects on the schoolchildren, something is very wrong. Such conduct by the Senate constitutes criminal action that endangers the lives and welfare of children. Their official behavior must be acknowledged for what it is — CRIMINAL — and prosecuted to the fullest extent of the law.
An Open Letter to Legislators Currently Considering Vaccine Legislation from Tetyana Obukhanych, PhD in Immunology
Re: VACCINE LEGISLATION
Dear Legislator:
My name is Tetyana Obukhanych. I hold a PhD in Immunology. I am writing this letter in the hope that it will correct several common misperceptions about vaccines in order to help you formulate a fair and balanced understanding that is supported by accepted vaccine theory and new scientific findings.
Do unvaccinated children pose a higher threat to the public than the vaccinated?
It is often stated that those who choose not to vaccinate their children for reasons of conscience endanger the rest of the public, and this is the rationale behind most of the legislation to end vaccine exemptions currently being considered by federal and state legislators country-wide. You should be aware that the nature of protection afforded by many modern vaccines – and that includes most of the vaccines recommended by the CDC for children – is not consistent with such a statement. I have outlined below the recommended vaccines that cannot prevent transmission of disease either because they are not designed to prevent the transmission of infection (rather, they are intended to prevent disease symptoms), or because they are for non-communicable diseases. People who have not received the vaccines mentioned below pose no higher threat to the general public than those who have, implying that discrimination against non-immunized children in a public school setting may not be warranted.
- IPV (inactivated poliovirus vaccine) cannot prevent transmission of poliovirus (see appendix for the scientific study, Item #1). Wild poliovirus has been non-existent in the USA for at least two decades. Even if wild poliovirus were to be re-imported by travel, vaccinating for polio with IPV cannot affect the safety of public spaces. Please note that wild poliovirus eradication is attributed to the use of a different vaccine, OPV or oral poliovirus vaccine. Despite being capable of preventing wild poliovirus transmission, use of OPV was phased out long ago in the USA and replaced with IPV due to safety concerns.
- Tetanus is not a contagious disease, but rather acquired from deep-puncture wounds contaminated with C. tetani spores. Vaccinating for tetanus (via the DTaP combination vaccine) cannot alter the safety of public spaces; it is intended to render personal protection only.
- While intended to prevent the disease-causing effects of the diphtheria toxin, the diphtheria toxoid vaccine (also contained in the DTaP vaccine) is not designed to prevent colonization and transmission of C. diphtheriae. Vaccinating for diphtheria cannot alter the safety of public spaces; it is likewise intended for personal protection only.
- The acellular pertussis (aP) vaccine (the final element of the DTaP combined vaccine), now in use in the USA, replaced the whole cell pertussis vaccine in the late 1990s, which was followed by an unprecedented resurgence of whooping cough. An experiment with deliberate pertussis infection in primates revealed that the aP vaccine is not capable of preventing colonization and transmission of B. pertussis (see appendix for the scientific study, Item #2). The FDA has issued a warning regarding this crucial finding.[1]
- Furthermore, the 2013 meeting of the Board of Scientific Counselors at the CDC revealed additional alarming data that pertussis variants (PRN-negative strains) currently circulating in the USA acquired a selective advantage to infect those who are up-to-date for their DTaP boosters (see appendix for the CDC document, Item #3), meaning that people who are up-to-date are more likely to be infected, and thus contagious, than people who are not vaccinated.
- Among numerous types of H. influenzae, the Hib vaccine covers only type b. Despite its sole intention to reduce symptomatic and asymptomatic (disease-less) Hib carriage, the introduction of the Hib vaccine has inadvertently shifted strain dominance towards other types of H. influenzae (types a through f).These types have been causing invasive disease of high severity and increasing incidence in adults in the era of Hib vaccination of children (see appendix for the scientific study, Item #4). The general population is more vulnerable to the invasive disease now than it was prior to the start of the Hib vaccination campaign. Discriminating against children who are not vaccinated for Hib does not make any scientific sense in the era of non-type b H. influenzae disease.
- Hepatitis B is a blood-borne virus. It does not spread in a community setting, especially among children who are unlikely to engage in high-risk behaviors, such as needle sharing or sex. Vaccinating children for hepatitis B cannot significantly alter the safety of public spaces. Further, school admission is not prohibited for children who are chronic hepatitis B carriers. To prohibit school admission for those who are simply unvaccinated – and do not even carry hepatitis B – would constitute unreasonable and illogical discrimination.
In summary, a person who is not vaccinated with IPV, DTaP, HepB, and Hib vaccines due to reasons of conscience poses no extra danger to the public than a person who is. No discrimination is warranted.
How often do serious vaccine adverse events happen?
It is often stated that vaccination rarely leads to serious adverse events. Unfortunately, this statement is not supported by science. A recent study done in Ontario, Canada, established thatvaccination actually leads to an emergency room visit for 1 in 168 children following their 12-month vaccination appointment and for 1 in 730 children following their 18-month vaccination appointment (see appendix for a scientific study, Item #5).
When the risk of an adverse event requiring an ER visit after well-baby vaccinations is demonstrably so high, vaccination must remain a choice for parents, who may understandably be unwilling to assume this immediate risk in order to protect their children from diseases that are generally considered mild or that their children may never be exposed to.
Can discrimination against families who oppose vaccines for reasons of conscience prevent future disease outbreaks of communicable viral diseases, such as measles?
Measles research scientists have for a long time been aware of the “measles paradox.” I quote from the article by Poland & Jacobson (1994) “Failure to Reach the Goal of Measles Elimination: Apparent Paradox of Measles Infections in Immunized Persons.” Arch Intern Med154:1815-1820:
“The apparent paradox is that as measles immunization rates rise to high levels in a population, measles becomes a disease of immunized persons.”[2]
Further research determined that behind the “measles paradox” is a fraction of the population called LOW VACCINE RESPONDERS. Low-responders are those who respond poorly to the first dose of the measles vaccine. These individuals then mount a weak immune response to subsequent RE-vaccination and quickly return to the pool of “susceptibles’’ within 2-5 years, despite being fully vaccinated.[3]
Re-vaccination cannot correct low-responsiveness: it appears to be an immuno-genetic trait.[4] The proportion of low-responders among children was estimated to be 4.7% in the USA.[5]
Studies of measles outbreaks in Quebec, Canada, and China attest that outbreaks of measles still happen, even when vaccination compliance is in the highest bracket (95-97% or even 99%, see appendix for scientific studies, Items #6&7). This is because even in high vaccine responders, vaccine-induced antibodies wane over time. Vaccine immunity does not equal life-long immunity acquired after natural exposure.
It has been documented that vaccinated persons who develop breakthrough measles are contagious. In fact, two major measles outbreaks in 2011 (in Quebec, Canada, and in New York, NY) were re-imported by previously vaccinated individuals.[6] – [7]
Taken together, these data make it apparent that elimination of vaccine exemptions, currently only utilized by a small percentage of families anyway, will neither solve the problem of disease resurgence nor prevent re-importation and outbreaks of previously eliminated diseases.
Is discrimination against conscientious vaccine objectors the only practical solution?
The majority of measles cases in recent US outbreaks (including the recent Disneyland outbreak) are adults and very young babies, whereas in the pre-vaccination era, measles occurred mainly between the ages 1 and 15. Natural exposure to measles was followed by lifelong immunity from re-infection, whereas vaccine immunity wanes over time, leaving adults unprotected by their childhood shots. Measles is more dangerous for infants and for adults than for school-aged children.
Despite high chances of exposure in the pre-vaccination era, measles practically never happened in babies much younger than one year of age due to the robust maternal immunity transfer mechanism. The vulnerability of very young babies to measles today is the direct outcome of the prolonged mass vaccination campaign of the past, during which their mothers, themselves vaccinated in their childhood, were not able to experience measles naturally at a safe school age and establish the lifelong immunity that would also be transferred to their babies and protect them from measles for the first year of life.
Luckily, a therapeutic backup exists to mimic now-eroded maternal immunity. Infants as well as other vulnerable or immunocompromised individuals, are eligible to receive immunoglobulin, a potentially life-saving measure that supplies antibodies directed against the virus to prevent or ameliorate disease upon exposure (see appendix, Item #8).
In summary: 1) due to the properties of modern vaccines, non-vaccinated individuals pose no greater risk of transmission of polio, diphtheria, pertussis, and numerous non-type b H. influenzae strains than vaccinated individuals do, non-vaccinated individuals pose virtually no danger of transmission of hepatitis B in a school setting, and tetanus is not transmissible at all; 2) there is a significantly elevated risk of emergency room visits after childhood vaccination appointments attesting that vaccination is not risk-free; 3) outbreaks of measles cannot be entirely prevented even if we had nearly perfect vaccination compliance; and 4) an effective method of preventing measles and other viral diseases in vaccine-ineligible infants and the immunocompromised, immunoglobulin, is available for those who may be exposed to these diseases.
Taken together, these four facts make it clear that discrimination in a public school setting against children who are not vaccinated for reasons of conscience is completely unwarranted as the vaccine status of conscientious objectors poses no undue public health risk.
Sincerely Yours,
~ Tetyana Obukhanych, PhD
Tetyana Obukhanych, PhD, is the author of the book Vaccine Illusion. She has studied immunology in some of the world’s most prestigious medical institutions. She earned her PhD in Immunology at the Rockefeller University in New York and did postdoctoral training at Harvard Medical School, Boston, MA and Stanford University in California.
Dr. Obukhanych offers online classes for those who want to gain deeper understanding of how the immune system works and whether the immunologic benefits of vaccines are worth the risks: Natural Immunity Fundamentals.
Appendix
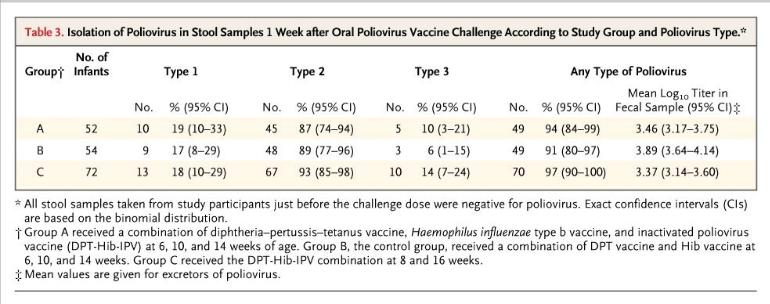
Item #1. The Cuba IPV Study collaborative group. (2007) Randomized controlled trial of inactivated poliovirus vaccine in Cuba. N Engl J Med 356:1536-44
http://www.ncbi.nlm.nih.gov/pubmed/17429085
The table below from the Cuban IPV study documents that 91% of children receiving no IPV (control group B) were colonized with live attenuated poliovirus upon deliberate experimental inoculation. Children who were vaccinated with IPV (groups A and C) were similarly colonized at the rate of 94-97%. High counts of live virus were recovered from the stool of children in all groups. These results make it clear that IPV cannot be relied upon for the control of polioviruses.
Item #2. Warfel et al. (2014) Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model.Proc Natl Acad Sci USA 111:787-92
http://www.ncbi.nlm.nih.gov/pubmed/24277828
“Baboons vaccinated with aP were protected from severe pertussis-associated symptoms but not from colonization, did not clear the infection faster than naïve [unvaccinated] animals, and readily transmitted B. pertussis to unvaccinated contacts. By comparison, previously infected [naturally-immune] animals were not colonized upon secondary infection.”
Item #3. Meeting of the Board of Scientific Counselors, Office of Infectious Diseases, Centers for Disease Control and Prevention, Tom Harkins Global Communication Center, Atlanta, Georgia, December 11-12, 2013
http://www.cdc.gov/maso/facm/pdfs/BSCOID/2013121112_BSCOID_Minutes.pdf
Resurgence of Pertussis (p.6)
“Findings indicated that 85% of the isolates [from six Enhanced Pertussis Surveillance Sites and from epidemics in Washington and Vermont in 2012] were PRN-deficient and vaccinated patients had significantly higher odds than unvaccinated patients of being infected with PRN-deficient strains. Moreover, when patients with up-to-date DTaP vaccinations were compared to unvaccinated patients, the odds of being infected with PRN-deficient strains increased, suggesting that PRN-bacteria may have a selective advantage in infecting DTaP-vaccinated persons.”
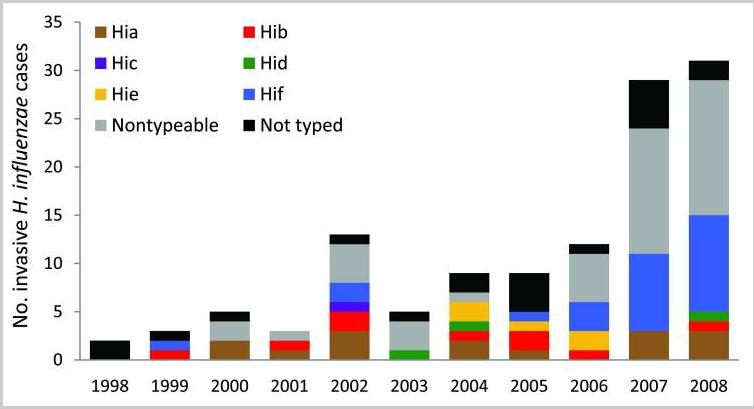
Item #4. Rubach et al. (2011) Increasing incidence of invasive Haemophilus influenzae disease in adults, Utah, USA. Emerg Infect Dis 17:1645-50
http://www.ncbi.nlm.nih.gov/pubmed/21888789
The chart below from Rubach et al. shows the number of invasive cases of H. influenzae(all types) in Utah in the decade of childhood vaccination for Hib.
Item #5. Wilson et al. (2011) Adverse events following 12 and 18 month vaccinations: a population-based, self-controlled case series analysis. PLoS One 6:e27897
http://www.ncbi.nlm.nih.gov/pubmed/22174753
“Four to 12 days post 12 month vaccination, children had a 1.33 (1.29-1.38) increased relative incidence of the combined endpoint compared to the control period, or at least one event during the risk interval for every 168 children vaccinated. Ten to 12 days post 18 month vaccination, the relative incidence was 1.25 (95%, 1.17-1.33) which represented at least one excess event for every 730 children vaccinated. The primary reason for increased events was statistically significant elevations in emergency room visits following all vaccinations.”
Item #6. De Serres et al. (2013) Largest measles epidemic in North America in a decade–Quebec, Canada, 2011: contribution of susceptibility, serendipity, and superspreading events. J Infect Dis 207:990-98
http://www.ncbi.nlm.nih.gov/pubmed/23264672
“The largest measles epidemic in North America in the last decade occurred in 2011 in Quebec, Canada.”
“A super-spreading event triggered by 1 importation resulted in sustained transmission and 678 cases.”
“The index case patient was a 30-39-year old adult, after returning to Canada from the Caribbean. The index case patient received measles vaccine in childhood.”
“Provincial [Quebec] vaccine coverage surveys conducted in 2006, 2008, and 2010 consistently showed that by 24 months of age, approximately 96% of children had received 1 dose and approximately 85% had received 2 doses of measles vaccine, increasing to 97% and 90%, respectively, by 28 months of age. With additional first and second doses administered between 28 and 59 months of age, population measles vaccine coverage is even higher by school entry.”
“Among adolescents, 22% [of measles cases] had received 2 vaccine doses. Outbreak investigation showed this proportion to have been an underestimate; active case finding identified 130% more cases among 2-dose recipients.”
Item #7. Wang et al. (2014) Difficulties in eliminating measles and controlling rubella and mumps: a cross-sectional study of a first measles and rubella vaccination and a second measles, mumps, and rubella vaccination. PLoS One9:e89361
http://www.ncbi.nlm.nih.gov/pubmed/24586717
“The reported coverage of the measles-mumps-rubella (MMR) vaccine is greater than 99.0% in Zhejiang province. However, the incidence of measles, mumps, and rubella remains high.”
Item #8. Immunoglobulin Handbook, Health Protection Agency
HUMAN NORMAL IMMUNOGLOBULIN (HNIG):
Indications
- To prevent or attenuate an attack in immuno-compromised contacts
- To prevent or attenuate an attack in pregnant women
- To prevent or attenuate an attack in infants under the age of 9 months
[1] http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm376937.htm
[2] http://archinte.jamanetwork.com/article.aspx?articleid=619215
[3] Poland (1998) Am J Hum Genet 62:215-220
http://www.ncbi.nlm.nih.gov/pubmed/9463343
“ ‘poor responders,’ who were re-immunized and developed poor or low-level antibody responses only to lose detectable antibody and develop measles on exposure 2–5 years later.”
[4] ibid
“Our ongoing studies suggest that seronegativity after vaccination [for measles] clusters among related family members, that genetic polymorphisms within the HLA [genes] significantly influence antibody levels.”
[5] LeBaron et al. (2007) Arch Pediatr Adolesc Med 161:294-301
http://www.ncbi.nlm.nih.gov/pubmed/17339511
“Titers fell significantly over time [after second MMR] for the study population overall and, by the final collection, 4.7% of children were potentially susceptible.”
[6] De Serres et al. (2013) J Infect Dis 207:990-998
http://www.ncbi.nlm.nih.gov/pubmed/23264672
“The index case patient received measles vaccine in childhood.”
[7]Rosen et al. (2014) Clin Infect Dis 58:1205-1210
http://www.ncbi.nlm.nih.gov/pubmed/24585562
“The index patient had 2 doses of measles-containing vaccine.”
Source: Aletho News
Na Engleskom jeziku LIJEČNICA dokazuje ALUMINIJ u cjepivu
“Nekad sam bila idiot.
Mislila sam da ljudi koji ne cijepe iskorištavaju one koji cijepe. Smatrala sam da su to privilegirani oportunisti. I…bila sam liječnik koji cijepi. Jer me nisu učili NIŠTA o cjepivima. Jer nikad nisam ni srela necijepljeno dijete. No jednom kad sam srela necijepljeno dijete i kad sam iz prve ruke počela primjećivati probleme kod svojih cijepljenih pacijenata…i počela sama istraživati, okrenula sam se za 180 stupnjeva. I upoznala sam liječnike koji to isto mogu učiniti. Neki od njih upravo zbog vas roditelja koji ste im predočili činjenice. Tiho, mirno i racionalno. To je ključ.”
Dr Humphries in Tampere, Finland, November 2015. Hear the arguments that pro-vaccine doctors make about aluminum (called aluminium in Europe), and the science (or lack there-of) behind it. Dr. Suzanne breaks down the issue of aluminum into fine detail to help you discuss this issue which is an Achilles heel in the vaccination argument.
Amerika platila 3 milijarde dolara odštete, RADI CJEPIVA!

VAKCINE ZA BEBE IZAZIVAJU AUTIZAM, TEŠKE BOLESTI I SMRT: Amerika platila 3 milijarde odštete!
Društvo 21:33, 13.03.2016. 12104

U 2015. godini – a sve su ovo najsvežiji zvanični podaci – u 509 slučajeva (posle tužbi) SAD su isplatile više od 204 miliona dolara. A u Srbiji? Nikom nije isplaćen ni dinar!
Novi zakon
Vakcinacija je u Srbiji odnedavno obavezna. Podsetimo, 24. februara, sa 156 glasova „za“, Skupština Srbije usvojila je Zakon o zaštiti stanovništva od zaraznih bolesti kojim je propisano da roditelji ili staratelji koji ne budu vakcinisali svoju decu budu kažnjeni novčano od 30.000 do 150.000 dinara, jer, kaže zakon, „nevakcinisano dete ugrožava život druge dece“.
– Beba koju sam rodila 2013. godine na porođaju je udahnula plodovu vodu, ali je lekarka procenila da je dovoljno zdrava i da može primiti vakcinu protiv hepatitisa B. Nakon vakcinacije stanje joj se naglo pogoršalo i šest dana kasnije je umrla. Zbog tog groznog iskustva odlučili smo da drugo dete ne vakcinišemo – odlučna je Beograđanka Ljiljana Kostić.

Ona se pita šta je zapravo cilj novčane kazne:
– Svejedno mi je da li je to pet ili sto pedeset hiljada dinara kazne ili nekakav prinudni rad, za koji sam čula da se pominje, meni je bitno da moje dete bude zdravo!
U Americi, međutim, vakcinacija je stvar ličnog izbora. A upravo u SAD, samo u prva dva meseca ove godine dokazano je 209 slučajeva zbog kojih je već isplaćen 81 milion dolara odštete unesrećenim porodicama!
„Ne eksperimentima! Naša deca nisu procenat“
RODITELJI IZAŠLI NA PROTEST
U znak oštrog protesta zbog najnovijih izmena zakona o obaveznoj vakcinaciji dece i uvođenja drakonskih kazni roditeljima koji odbijaju poslušnost, veliki broj roditelja i građana okupio se u subotu na Trgu Republike kako bi odlučno rekli: „Ne, eksperimentima! Naša deca nisu procenat!“ U organizaciji UG Građanska inicijativa za neobaveznu vakcinaciju, ovo je bio najposećeniji skup do sada. Govornici su ukazali na štetnost od vakcina i nesrazmerno prilagođavanje zakona Srbije i EU, gde obavezna vakcinacija, inače, ne postoji.
MMR i autizam
Devedesetih godina prošlog veka povela se žestoka diskusija o mogućnosti pojave autizma kod dece prilikom primanja vakcine MMR (cepivo protiv rubeola, malih boginja i zaušaka), koju je pratio niz publikacija i studija koje su tvrdile da ta veza postoji. Ustanovljeno je da se autizam javlja kod dece koja prime MMR vakcinu u rasponu od 0,7 do 21,1 odsto na 10.000 vakcinisanih (u proseku 5,2 dece na 10.000 vakcinisanih).
– Vakcinacija je veoma uspešna zaštita od mnoštva opasnih zaraznih bolesti. Ne treba se bojati vakcinacije, treba se bojati zaraznih bolesti od kojih se štitimo vakcinacijom. Zapravo, ni njih se više ne treba bojati, dokle god imamo vakcinaciju kao preventivnu metodu – tvrdi dr Srđa Janković, imunolog na Univerzitetskoj dečjoj klinici u Tiršovoj.

Upravo je to i stav Svetske zdravstvene organizacije: zdravu decu bi trebalo vakcinisati. SZO, telo Ujedinjenih nacija, u izveštaju iz 2013. insistira na odlaganju vakcinacije ukoliko su deca prehlađena ili izložena bilo kom vidu upale organa za varenje.
Dakle, poenta čitave priče „za i protiv vakcinacije“ svodi se na to da većina lekara u svetu tvrdi da vakcinacija nije opasna ni po život ni po zdravlje deteta, ali da je od krucijalnog značaja da dete bude apsolutno zdravo da bi bilo vakcinisano. I to je, kažu, cela suština.
Činjenice
Kalendar obavezne vakcinacije u Srbiji
1 Be-se-že vakcina: na rođenju ili tokom prve godine života
2 Hepatitis B vakcina se daje u tri doze: na rođenju, sa 1 mesec i sa 6 meseci
3 Vakcina protiv 5 bolesti (protiv difterije, tetanusa, pertusisa, dečje paralize i hemofilus influence tip B) daje se sa 2 meseca, 3 i po meseca i 5 meseci
a) Prva revakcinacija protiv 4 bolesti (difterije, tetanusa, pertusisa i dečje paralize) vrši se 10-12 meseci nakon poslednje doze
b) Druga revakcinacija protiv 4 bolesti (difterije, tetanusa, pertusisa i polija) vrši se sa 6 godina, tj. pred polazak u školu
c) treća revakcinacija protiv 3 bolesti (difterije, tetanusa i dečje paralize) obavlja se sa 14 godina
4 Vakcina MMR (male boginje, zauške, rubeole) – sa 12 meseci i sa 6 godina pred polazak u školu
*Izvor: GAK Narodni front
U sutrašnjem broju čitajte: Ko je u Srbiji glasao protiv vakcinacije i šta kaže Lekarska komora
Pratite KURIR na VIBERU: http://chats.viber.com/kurir
Autor: Istarživački biro
Baš SVE o štetnosti CJEPIVA.

Projekt “Cijepljenje – pravo izbora” pokrenula je Hrvatska udruga za promicanje prava pacijenata (HUZPPP). Skraćeni naziv Udruge je Hrvatska udruga za prava pacijenata.
Za provedbu projekta zadužena je radna grupa Udruge pod nazivom Sloboda odlučivanja za obavezno cijepljenje djece, koja od veljače 2014. godine u javnosti djeluje pod imenom Građanska inicijativa Cijepljenje – pravo izbora.
Glavni cilj projekta je postizanje neobaveznog cijepljenja u Hrvatskoj, a obrazložen je u niže istaknutoj Izjavi Hrvatske udruga za promicanje prava pacijenata koja sadrži temeljne pravne i etičke razloge za uvođenje neobaveznog (preporučenog) cijepljenja.
Projekt je započeo u studenom 2014. godine*, a predviđeno trajanje je do ispunjenjaciljeva.Ciljevi projekta ostvaruju se kroz niz aktivnosti te putem potpora.
* I prije službenog početka projekta, već 2. veljače 2014. na Facebooku je pokrenuta stranica (zajednica) Cijepljenje – pravo izbora.

Izjava Hrvatske udruge za promicanje prava pacijenata
Hrvatska udruga za promicanje prava pacijenata zastupa stav kako je obaveza cijepljenja neutemeljena te pogrešno postavljena i provođena iz sljedećih razloga:
1. Cijepljenje je preventivna medicinska usluga te kao i sve druge medicinske usluge(kurativne, preventivne i druge) stoji na raspolaganju zainteresiranima, koji nakon što budu propisno informirani o istome, moraju moći potpuno slobodno donijeti odluku o prihvaćanju ili odbijanju iste – ovo TEMELJNO LJUDSKO PRAVO I PRAVO PACIJENTA (priznato brojnim međunarodnim konvencijama) se trenutačno u Republici Hrvatskoj grubo krši, budući da je glavna svrha slobodnog i informiranog pristanka potvrditi autonomiju pacijenta, promovirati njegovo pravo na samoodređenje i osigurati poštivanje ljudskog dostojanstva svakog pacijenta. Donošenje odluka i sudjelovanje u donošenju odluka o vlastitom zdravlju priznaju se danas kao pacijentovo ljudsko pravo i od toga prava Hrvatska udruga za promicanje prava pacijenata jednostavno ne može i neće odustati.;
2. Opisanom praksom podriva se i povjerenje u odnosu liječnik-pacijent, krši se liječnička etika te se sveukupno smanjuje povjerenje u zdravstveni sustav. Brojni zdravstveni djelatnici nalaze se između međusobno suprotstavljenih zakonskih odredbi, pri čemu su izloženi prekršajnim i drugim represivnim mjerama čime je i njihova pozicija ovaj čas neopravdano izložena različitim pravnim rizicima (dakle nisu samo ugrožena prava roditelja i djece, nego i brojnih zdravstvenih djelatnika).;
3. Sukladno važećim propisima, ali i temeljem prirodnog prava, nesporno je da isključivo roditelji, mogu slobodno donijeti konkretnu odluku glede svojeg djeteta, na način za koji ti roditelji smatraju da je u najboljem interesu djeteta. Čak i slučajevima u kojima su sukladno Obiteljskom zakonu pojedinim roditeljima ograničena ili oduzeta roditeljska prava, tada konkretnu odluku slobodno donosi posebni skrbnik djeteta, a to ni u kojem slučaju nije ovlašten činiti primjerice Ministar zdravlja, temeljem svoje pozicije nositelja jednog dijela izvršne vlasti ili netko treći, osim ranije spomenutih zakonskih zastupnika svakog djeteta. Nažalost, trenutačno se u Republici Hrvatskoj izravno krše temeljna ljudska prava brojnih roditelja i djece, čija se slobodna odluka, uvjerenje i/ili prijašnje iskustvo ne podudara s tako zvanim “obveznim cijepljenjem”.;
4. Nesporno je kako je pravo djeteta da bude u poziciji da mu je omogućeno primiti bilo koje ili sva medicinskom strukom preporučena cjepiva, ali nikako ne može biti ispravno smatrati pravom djeteta da bude cijepljeno bez slobodne odluke roditelja o tome je li ta preporuka za njihovo dijete prihvatljiv razlog da prihvate ponuđenu uslugu cijepljenja svojega djeteta.
U RH je Zakonom o zaštiti pučanstva od zaraznih bolesti propisana obaveza cijepljenja. Način i razlozi na koji je cijepljenje postalo zakonskom obavezom seže u daleku prošlost u kojoj su dotične zarazne bolesti bile toliko velika prijetnja da je sukladno mišljenju medicinske struke to doista tada bilo smatrano najboljim načinom odbrane od tih bolesti i njihovih posljedica. No, nakon što su se te bolesti stavile pod nadzor i više nisu predstavljale toliku značajnu opasnost za ukupno društvo, a društvo postalo dovoljno pismeno i dostupnih obavijesti, obavezu cijepljenja više ne možemo smatrati preporukom medicinske struke te se medicinski stručnjaci o tome na takav način i očituju. Unatoč tome, nema odgovora politike na njihova izravna izjašnjavanja o tome da ne vide baš nekih razloga da cijepljenje bude obavezno, ali da svakako ima preporuku struke.
Koristeći se represivnim mjerama prema zdravstvenim radnicima i stanovništvu politika i nadalje zadržava pravo ograničavanja ljudskih sloboda, iako viši interesi više ne mogu dobiti potporu struke niti zaštitnika ljudskih prava. Sasvim je razvidno kako se time ujedno zadire i u slobodu tržišta, a temeljem brojnih dokaza o vrlo visokom stupnju korupcije u svim društvima upravo u sferi zdravstva, ustrajanje na zakonskoj obavezi cijepljenja podriva zdravstveni sustav sa svih strana: od onih koji kroje nacionalnu zdravstvenu politiku do medicinskih stručnjaka.;
 mr. sci. Đula Rušinović-Sunara, dr. med.
mr. sci. Đula Rušinović-Sunara, dr. med.
5. Nesporno je da zakonski zastupnici djeteta nisu nepogrešivi i da imaju pravo slobodno donijeti odluku, koja će se možda nekada u budućnosti pokazati kao pogrešnom, bilo da im dijete oboli od neke bolesti, koja se možda mogla spriječiti cijepljenjem (kažemo “možda” jer nijedan proizvođač cjepiva u svojim uputama o lijeku ne jamči da je zaštita koju oni pružaju stopostotna niti da je vremenski neograničena), bilo da im dijete pretrpi neki oblik teške nuspojave, koje se nažalost znaju pojaviti uz svaki lijek, ili da im uslijed jednog ili više cjepiva, možda i uz doprinos drugih faktora, zdravstveno stanje djeteta bude trajno i teško narušeno. Iskustva su različita, isto kao što su različita i djeca i njihov imunitet i genetika, njihova prehrana, i različiti brojni drugi štetni ili korisni faktori kojima su djeca izložena u svakodnevnom životu.;
6. Ne kažemo da ne postoji niti jedan dobar razlog za cijepljenje od pojedinih zaraznih bolesti, ali uvjereni smo da ne postoji niti jedan dobar razlog za represivno nametanje bilo kakvog preventivnog ili kurativnog medicinskog postupka, a naročito određenog cjepiva, jer isto predstavlja prisilno unošenja stranog tijela u slobodno ljudsko biće, a što jest i što uvijek mora biti nedopustivo bez prethodne slobodne i informirane privole.
mr. sci. Đula Rušinović-Sunara, dr. med., specijalistica opće kirugije, predsjednica Hrvatske udruge za promicanje prava pacijenata
Share this article
Na Engleskom, sa Harwarda DOKAZI štetnosti cjepiva.
Harvard Trained Immunologist Demolishes California Legislation That Terminates Vaccine Exemptions
The following open letter by a PhD Immunologist completely demolishes the current California legislative initiative to remove all vaccine exemptions. That such a draconian and cynical state statute is under consideration in the ‘Golden State’ is as shocking as it is predictable. After all, it was mysteriously written and submitted shortly after the manufactured-in-Disneyland measles ‘outbreak’.
The indisputable science that is employed by Tetyana Obukhanych, PhD ought to be read by every CA legislator who is entertaining an affirmative vote for SB277. Dr. Obukhanych skillfully deconstructs the many false and fabricated arguments that are advanced by Big Pharma and the U.S Federal Government as they attempt to implement a nationwide Super-Vaccination agenda.
When the California Senate refuses to consider authoritative scientific evidence which categorically proves the dangerous vaccine side effects on the schoolchildren, something is very wrong. Such conduct by the Senate constitutes criminal action that endangers the lives and welfare of children. Their official behavior must be acknowledged for what it is — CRIMINAL — and prosecuted to the fullest extent of the law.
An Open Letter to Legislators Currently Considering Vaccine Legislation from Tetyana Obukhanych, PhD in Immunology
Re: VACCINE LEGISLATION
Dear Legislator:
My name is Tetyana Obukhanych. I hold a PhD in Immunology. I am writing this letter in the hope that it will correct several common misperceptions about vaccines in order to help you formulate a fair and balanced understanding that is supported by accepted vaccine theory and new scientific findings.
Do unvaccinated children pose a higher threat to the public than the vaccinated?
It is often stated that those who choose not to vaccinate their children for reasons of conscience endanger the rest of the public, and this is the rationale behind most of the legislation to end vaccine exemptions currently being considered by federal and state legislators country-wide. You should be aware that the nature of protection afforded by many modern vaccines – and that includes most of the vaccines recommended by the CDC for children – is not consistent with such a statement. I have outlined below the recommended vaccines that cannot prevent transmission of disease either because they are not designed to prevent the transmission of infection (rather, they are intended to prevent disease symptoms), or because they are for non-communicable diseases. People who have not received the vaccines mentioned below pose no higher threat to the general public than those who have, implying that discrimination against non-immunized children in a public school setting may not be warranted.
- IPV (inactivated poliovirus vaccine) cannot prevent transmission of poliovirus (see appendix for the scientific study, Item #1). Wild poliovirus has been non-existent in the USA for at least two decades. Even if wild poliovirus were to be re-imported by travel, vaccinating for polio with IPV cannot affect the safety of public spaces. Please note that wild poliovirus eradication is attributed to the use of a different vaccine, OPV or oral poliovirus vaccine. Despite being capable of preventing wild poliovirus transmission, use of OPV was phased out long ago in the USA and replaced with IPV due to safety concerns.
- Tetanus is not a contagious disease, but rather acquired from deep-puncture wounds contaminated with C. tetani spores. Vaccinating for tetanus (via the DTaP combination vaccine) cannot alter the safety of public spaces; it is intended to render personal protection only.
- While intended to prevent the disease-causing effects of the diphtheria toxin, the diphtheria toxoid vaccine (also contained in the DTaP vaccine) is not designed to prevent colonization and transmission of C. diphtheriae. Vaccinating for diphtheria cannot alter the safety of public spaces; it is likewise intended for personal protection only.
- The acellular pertussis (aP) vaccine (the final element of the DTaP combined vaccine), now in use in the USA, replaced the whole cell pertussis vaccine in the late 1990s, which was followed by an unprecedented resurgence of whooping cough. An experiment with deliberate pertussis infection in primates revealed that the aP vaccine is not capable of preventing colonization and transmission of B. pertussis (see appendix for the scientific study, Item #2). The FDA has issued a warning regarding this crucial finding.[1]
- Furthermore, the 2013 meeting of the Board of Scientific Counselors at the CDC revealed additional alarming data that pertussis variants (PRN-negative strains) currently circulating in the USA acquired a selective advantage to infect those who are up-to-date for their DTaP boosters (see appendix for the CDC document, Item #3), meaning that people who are up-to-date are more likely to be infected, and thus contagious, than people who are not vaccinated.
- Among numerous types of H. influenzae, the Hib vaccine covers only type b. Despite its sole intention to reduce symptomatic and asymptomatic (disease-less) Hib carriage, the introduction of the Hib vaccine has inadvertently shifted strain dominance towards other types of H. influenzae (types a through f).These types have been causing invasive disease of high severity and increasing incidence in adults in the era of Hib vaccination of children (see appendix for the scientific study, Item #4). The general population is more vulnerable to the invasive disease now than it was prior to the start of the Hib vaccination campaign. Discriminating against children who are not vaccinated for Hib does not make any scientific sense in the era of non-type b H. influenzae disease.
- Hepatitis B is a blood-borne virus. It does not spread in a community setting, especially among children who are unlikely to engage in high-risk behaviors, such as needle sharing or sex. Vaccinating children for hepatitis B cannot significantly alter the safety of public spaces. Further, school admission is not prohibited for children who are chronic hepatitis B carriers. To prohibit school admission for those who are simply unvaccinated – and do not even carry hepatitis B – would constitute unreasonable and illogical discrimination.
In summary, a person who is not vaccinated with IPV, DTaP, HepB, and Hib vaccines due to reasons of conscience poses no extra danger to the public than a person who is. No discrimination is warranted.
How often do serious vaccine adverse events happen?
It is often stated that vaccination rarely leads to serious adverse events. Unfortunately, this statement is not supported by science. A recent study done in Ontario, Canada, established thatvaccination actually leads to an emergency room visit for 1 in 168 children following their 12-month vaccination appointment and for 1 in 730 children following their 18-month vaccination appointment (see appendix for a scientific study, Item #5).
When the risk of an adverse event requiring an ER visit after well-baby vaccinations is demonstrably so high, vaccination must remain a choice for parents, who may understandably be unwilling to assume this immediate risk in order to protect their children from diseases that are generally considered mild or that their children may never be exposed to.
Can discrimination against families who oppose vaccines for reasons of conscience prevent future disease outbreaks of communicable viral diseases, such as measles?
Measles research scientists have for a long time been aware of the “measles paradox.” I quote from the article by Poland & Jacobson (1994) “Failure to Reach the Goal of Measles Elimination: Apparent Paradox of Measles Infections in Immunized Persons.” Arch Intern Med154:1815-1820:
“The apparent paradox is that as measles immunization rates rise to high levels in a population, measles becomes a disease of immunized persons.”[2]
Further research determined that behind the “measles paradox” is a fraction of the population called LOW VACCINE RESPONDERS. Low-responders are those who respond poorly to the first dose of the measles vaccine. These individuals then mount a weak immune response to subsequent RE-vaccination and quickly return to the pool of “susceptibles’’ within 2-5 years, despite being fully vaccinated.[3]
Re-vaccination cannot correct low-responsiveness: it appears to be an immuno-genetic trait.[4] The proportion of low-responders among children was estimated to be 4.7% in the USA.[5]
Studies of measles outbreaks in Quebec, Canada, and China attest that outbreaks of measles still happen, even when vaccination compliance is in the highest bracket (95-97% or even 99%, see appendix for scientific studies, Items #6&7). This is because even in high vaccine responders, vaccine-induced antibodies wane over time. Vaccine immunity does not equal life-long immunity acquired after natural exposure.
It has been documented that vaccinated persons who develop breakthrough measles are contagious. In fact, two major measles outbreaks in 2011 (in Quebec, Canada, and in New York, NY) were re-imported by previously vaccinated individuals.[6] – [7]
Taken together, these data make it apparent that elimination of vaccine exemptions, currently only utilized by a small percentage of families anyway, will neither solve the problem of disease resurgence nor prevent re-importation and outbreaks of previously eliminated diseases.
Is discrimination against conscientious vaccine objectors the only practical solution?
The majority of measles cases in recent US outbreaks (including the recent Disneyland outbreak) are adults and very young babies, whereas in the pre-vaccination era, measles occurred mainly between the ages 1 and 15. Natural exposure to measles was followed by lifelong immunity from re-infection, whereas vaccine immunity wanes over time, leaving adults unprotected by their childhood shots. Measles is more dangerous for infants and for adults than for school-aged children.
Despite high chances of exposure in the pre-vaccination era, measles practically never happened in babies much younger than one year of age due to the robust maternal immunity transfer mechanism. The vulnerability of very young babies to measles today is the direct outcome of the prolonged mass vaccination campaign of the past, during which their mothers, themselves vaccinated in their childhood, were not able to experience measles naturally at a safe school age and establish the lifelong immunity that would also be transferred to their babies and protect them from measles for the first year of life.
Luckily, a therapeutic backup exists to mimic now-eroded maternal immunity. Infants as well as other vulnerable or immunocompromised individuals, are eligible to receive immunoglobulin, a potentially life-saving measure that supplies antibodies directed against the virus to prevent or ameliorate disease upon exposure (see appendix, Item #8).
In summary: 1) due to the properties of modern vaccines, non-vaccinated individuals pose no greater risk of transmission of polio, diphtheria, pertussis, and numerous non-type b H. influenzae strains than vaccinated individuals do, non-vaccinated individuals pose virtually no danger of transmission of hepatitis B in a school setting, and tetanus is not transmissible at all; 2) there is a significantly elevated risk of emergency room visits after childhood vaccination appointments attesting that vaccination is not risk-free; 3) outbreaks of measles cannot be entirely prevented even if we had nearly perfect vaccination compliance; and 4) an effective method of preventing measles and other viral diseases in vaccine-ineligible infants and the immunocompromised, immunoglobulin, is available for those who may be exposed to these diseases.
Taken together, these four facts make it clear that discrimination in a public school setting against children who are not vaccinated for reasons of conscience is completely unwarranted as the vaccine status of conscientious objectors poses no undue public health risk.
Sincerely Yours,
~ Tetyana Obukhanych, PhD
Tetyana Obukhanych, PhD, is the author of the book Vaccine Illusion. She has studied immunology in some of the world’s most prestigious medical institutions. She earned her PhD in Immunology at the Rockefeller University in New York and did postdoctoral training at Harvard Medical School, Boston, MA and Stanford University in California.
Dr. Obukhanych offers online classes for those who want to gain deeper understanding of how the immune system works and whether the immunologic benefits of vaccines are worth the risks: Natural Immunity Fundamentals.
Appendix
Item #1. The Cuba IPV Study collaborative group. (2007) Randomized controlled trial of inactivated poliovirus vaccine in Cuba. N Engl J Med 356:1536-44
http://www.ncbi.nlm.nih.gov/pubmed/17429085
The table below from the Cuban IPV study documents that 91% of children receiving no IPV (control group B) were colonized with live attenuated poliovirus upon deliberate experimental inoculation. Children who were vaccinated with IPV (groups A and C) were similarly colonized at the rate of 94-97%. High counts of live virus were recovered from the stool of children in all groups. These results make it clear that IPV cannot be relied upon for the control of polioviruses.
Item #2. Warfel et al. (2014) Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model.Proc Natl Acad Sci USA 111:787-92
http://www.ncbi.nlm.nih.gov/pubmed/24277828
“Baboons vaccinated with aP were protected from severe pertussis-associated symptoms but not from colonization, did not clear the infection faster than naïve [unvaccinated] animals, and readily transmitted B. pertussis to unvaccinated contacts. By comparison, previously infected [naturally-immune] animals were not colonized upon secondary infection.”
Item #3. Meeting of the Board of Scientific Counselors, Office of Infectious Diseases, Centers for Disease Control and Prevention, Tom Harkins Global Communication Center, Atlanta, Georgia, December 11-12, 2013
http://www.cdc.gov/maso/facm/pdfs/BSCOID/2013121112_BSCOID_Minutes.pdf
Resurgence of Pertussis (p.6)
“Findings indicated that 85% of the isolates [from six Enhanced Pertussis Surveillance Sites and from epidemics in Washington and Vermont in 2012] were PRN-deficient and vaccinated patients had significantly higher odds than unvaccinated patients of being infected with PRN-deficient strains. Moreover, when patients with up-to-date DTaP vaccinations were compared to unvaccinated patients, the odds of being infected with PRN-deficient strains increased, suggesting that PRN-bacteria may have a selective advantage in infecting DTaP-vaccinated persons.”
Item #4. Rubach et al. (2011) Increasing incidence of invasive Haemophilus influenzae disease in adults, Utah, USA. Emerg Infect Dis 17:1645-50
http://www.ncbi.nlm.nih.gov/pubmed/21888789
The chart below from Rubach et al. shows the number of invasive cases of H. influenzae(all types) in Utah in the decade of childhood vaccination for Hib.
Item #5. Wilson et al. (2011) Adverse events following 12 and 18 month vaccinations: a population-based, self-controlled case series analysis. PLoS One 6:e27897
http://www.ncbi.nlm.nih.gov/pubmed/22174753
“Four to 12 days post 12 month vaccination, children had a 1.33 (1.29-1.38) increased relative incidence of the combined endpoint compared to the control period, or at least one event during the risk interval for every 168 children vaccinated. Ten to 12 days post 18 month vaccination, the relative incidence was 1.25 (95%, 1.17-1.33) which represented at least one excess event for every 730 children vaccinated. The primary reason for increased events was statistically significant elevations in emergency room visits following all vaccinations.”
Item #6. De Serres et al. (2013) Largest measles epidemic in North America in a decade–Quebec, Canada, 2011: contribution of susceptibility, serendipity, and superspreading events. J Infect Dis 207:990-98
http://www.ncbi.nlm.nih.gov/pubmed/23264672
“The largest measles epidemic in North America in the last decade occurred in 2011 in Quebec, Canada.”
“A super-spreading event triggered by 1 importation resulted in sustained transmission and 678 cases.”
“The index case patient was a 30-39-year old adult, after returning to Canada from the Caribbean. The index case patient received measles vaccine in childhood.”
“Provincial [Quebec] vaccine coverage surveys conducted in 2006, 2008, and 2010 consistently showed that by 24 months of age, approximately 96% of children had received 1 dose and approximately 85% had received 2 doses of measles vaccine, increasing to 97% and 90%, respectively, by 28 months of age. With additional first and second doses administered between 28 and 59 months of age, population measles vaccine coverage is even higher by school entry.”
“Among adolescents, 22% [of measles cases] had received 2 vaccine doses. Outbreak investigation showed this proportion to have been an underestimate; active case finding identified 130% more cases among 2-dose recipients.”
Item #7. Wang et al. (2014) Difficulties in eliminating measles and controlling rubella and mumps: a cross-sectional study of a first measles and rubella vaccination and a second measles, mumps, and rubella vaccination. PLoS One9:e89361
http://www.ncbi.nlm.nih.gov/pubmed/24586717
“The reported coverage of the measles-mumps-rubella (MMR) vaccine is greater than 99.0% in Zhejiang province. However, the incidence of measles, mumps, and rubella remains high.”
Item #8. Immunoglobulin Handbook, Health Protection Agency
HUMAN NORMAL IMMUNOGLOBULIN (HNIG):
Indications
- To prevent or attenuate an attack in immuno-compromised contacts
- To prevent or attenuate an attack in pregnant women
- To prevent or attenuate an attack in infants under the age of 9 months
[1] http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm376937.htm
[2] http://archinte.jamanetwork.com/article.aspx?articleid=619215
[3] Poland (1998) Am J Hum Genet 62:215-220
http://www.ncbi.nlm.nih.gov/pubmed/9463343
“ ‘poor responders,’ who were re-immunized and developed poor or low-level antibody responses only to lose detectable antibody and develop measles on exposure 2–5 years later.”
[4] ibid
“Our ongoing studies suggest that seronegativity after vaccination [for measles] clusters among related family members, that genetic polymorphisms within the HLA [genes] significantly influence antibody levels.”
[5] LeBaron et al. (2007) Arch Pediatr Adolesc Med 161:294-301
http://www.ncbi.nlm.nih.gov/pubmed/17339511
“Titers fell significantly over time [after second MMR] for the study population overall and, by the final collection, 4.7% of children were potentially susceptible.”
[6] De Serres et al. (2013) J Infect Dis 207:990-998
http://www.ncbi.nlm.nih.gov/pubmed/23264672
“The index case patient received measles vaccine in childhood.”
[7]Rosen et al. (2014) Clin Infect Dis 58:1205-1210
http://www.ncbi.nlm.nih.gov/pubmed/24585562
“The index patient had 2 doses of measles-containing vaccine.”
Source: Aletho News
¤
¤
SENZACIONALNO PRIZNANJE NAMOĆNIJE MEDICINSKE USTANOVE NA SVETU: FDA priznala da vakcine uzrokuju autizam
http://platform.twitter.com/widgets/tweet_button.64a917b4a230f163048902c783e1530f.sr.html#dnt=true&id=twitter-widget-0&lang=sr&original_referer=http%3A%2F%2Fwebtribune.rs%2Fsenzacionalno-priznanje-namocnije-medicinske-ustanove-na-svetu-fda-priznala-da-vakcine-uzrokuju-autizam%2F%23&size=m&text=SENZACIONALNO%20PRIZNANJE%20NAMO%C4%86NIJE%20MEDICINSKE%20USTANOVE%20NA%20SVETU%3A%20FDA%20priznala%20da%20vakcine%20uzrokuju%20autizam&time=1459704459000&type=share&url=http%3A%2F%2Fwebtribune.rs%2Fsenzacionalno-priznanje-namocnije-medicinske-ustanove-na-svetu-fda-priznala-da-vakcine-uzrokuju-autizam%2F39
.
Mejnstrim mediji su do sada uglavnom zataškavali ovakve dokumente, ali ovaj dokument je objavljen za javnost i eksplicitno navodi sve ono o čemu mnogi već duže vreme pričaju.

Administracija za hranu i lekove (FDA) je po prvi put priznala da vakcine uzrokuju autizam u dokumentu na njihovom sajtu.
U dokumentu se nalazi uputstvo za korišćenje vakcine Tripedia i eksplicitno se navodi da ona može uzrokovati „idiopatsku trombocitopeničnu purpuru, SIDS, anafilaktičku reakciju, celulitis, autizam, grčeve, encefalopatiju, hipotoniju, neuropatiju, pospanost i apneju“, piše jedan od najpoznatijih alternativnih sajtova na svetu “naturalnews.com”
Mejnstrim mediji su do sada uglavnom zataškavali ovakve dokumente, ali ovaj dokument je objavljen za javnost i eksplicitno navodi sve ono o čemu mnogi već duže vreme pričaju.
Živimo u mračnom dobu medicine kada vlada jaka cenzura i zastrašuju se svi oni koji se usude da išta progovore o vakcinama.
U mnogim slučajevima vakcine uzrokuju iste te slučajeve zbog kojih se navodno primenjuju, zbog čega dolazi do toga da epidemiju pokrenu upravo deca koja su vakcinisana.
Toksini iz vakcina slabe imuni sistem dece i čine ih nosiocem virusa iz same vakcine.
Vakcine danas ne postoje da bi lečile bolesti, već da bi stvarale profit. One mogu da stvore profit samo ako nemaju efekat, jer da imaju, niko se više ne bi razboljevao. Što je više vakcina, to je više bolesti i to se više širi panika u medijima da što više ljudi vakciniše svoju decu. I tako se ciklus ponavlja. Nauka o vakcinama je zapravo samo jedna ogromna marketinška šema i nema nikakve veze sa pravom naukom.
Jednog dana će se ta istina u potpunosti razotkriti i svi će tražiti od industrije vakcina da se povuče jednom za svagda pre nego što uništi ljudsku civilizaciju.
Webtribune.rs

